
Abstract
“Johnny, were you playing ball in the house?” your mom asks as you and she stare at the broken vase on the floor. Have you ever noticed your heart starting to pound just before telling a lie? It turns out that the body, not only the brain, can bring up emotions to influence our decisions. A racing heartbeat and sweaty palms, just before you do something risky, could be your body warning you about your upcoming actions. Scientists have discovered that our thoughts and emotions interact with our bodies to influence the decisions we make—often without our awareness. This phenomenon is called the somatic marker hypothesis. In this article, using the famous story of Phineas Gage, we explain how various brain areas work together with the body to generate a real-life “spidey-sense”!
Introduction
Have you ever had the feeling that one decision was better than another, or that something bad was going to happen, without really knowing why? Like when you have a bad feeling about taking a shortcut through your neighbor’s backyard rather than taking the long way home? It turns out our brains are constantly storing information from our environments and using that information to guide our actions. We also retain the feelings from our bodies—like a pounding heart when we are scared by our neighbor’s angry dog. Those feelings can come up again when we are faced with similar situations. Re-experiencing feelings from previous choices allows us to learn from our actions so that we know what to do the next time we are in a similar situation. In fact, our emotions, just like the situations we are in, can influence the decisions we make. In this way, our brains and our bodies interact to influence our behaviors. Together, they act like our very own “spidey-sense.”
But how do we learn to make good decisions? What brain areas are involved? How do emotions influence the ability to make decisions? Phineas Gage’s story can help us answer these questions.
Phineas Gage And The Ventromedial Prefrontal Cortex
In the 1800s, scientists started to learn what brain areas are involved in making good decisions from a remarkable case of a railroad worker named Phineas Gage. In 1848, Gage was working on railroad tracks when a metal rod he used to tamp dynamite accidently set off the powder, which shot the rod through the front of his head (Figure 1). Amazingly, he survived. After the accident, Gage could still walk and talk, but his friends said “Gage was no longer Gage” [1]. His personality seemed to have completely changed; he was once a hard-working and responsible man, but following the accident, he was described as irritable, disrespectful, and unreliable. He would quit new jobs, throw tantrums, get into fights, and seemed to not care about anyone or anything. Gage kept making bad decisions, which often got him into trouble.
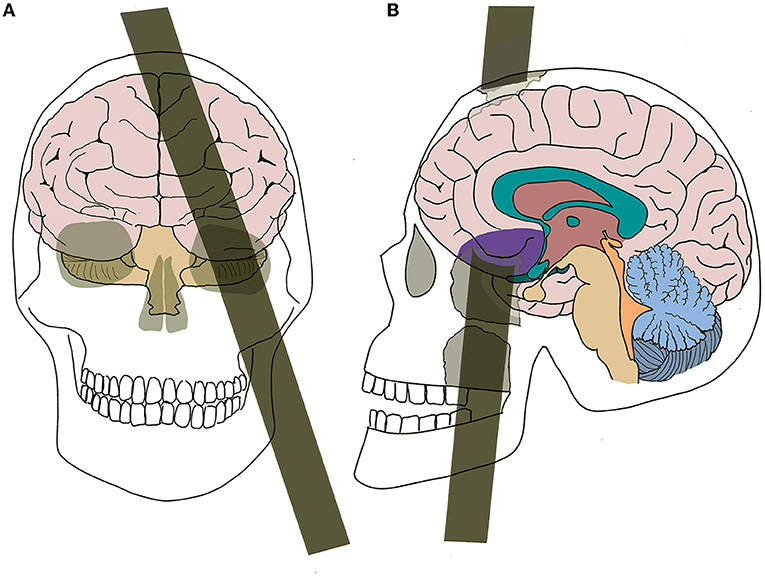
- Figure 1 - (A) A face view of how Phineas Gage’s metal tamping pole passed through his cheek and out the top of his head.
- (B) The metal tamping pole passed through the vmPFC region of Phineas Gage’s brain (purple).
The personality changes after his accident led scientists to believe that the metal rod had injured an important brain area—the ventromedial prefrontal cortex (vmPFC) [1]. Years later, scientists noticed similar changes in others with vmPFC damage. Those people also showed dramatic personality changes, like the inability to keep a steady job or manage their daily schedules, a lack of consideration for others, and a lack of thought about future consequences. Scientists wanted to understand how vmPFC damage leads to the behavioral changes and poor choices they observed.
Scientists found that people with vmPFC damage did not show impairments in memory or IQ tests. Then, scientists designed a task to assess good decision-making: the Iowa Gambling Task (IGT) [1—3] (Figure 2). In this task, people are told to try to make as much money as possible by choosing from several decks of cards. Each deck is associated with various amounts of wins and losses. “Good” decks have small wins and small losses, and at the end of the game, players usually leave with money. “Bad” decks have big wins and big losses, and at the end of the game, players leave with nothing. By the end of the task, people without vmPFC damage can usually say which are the “good” and “bad” decks [2—3]. Scientists noticed three interesting things in these people when they played the IGT. First, they switch to playing mostly from the “good” decks after losing large sums of money on the “bad” decks; second, this shift to the “good” decks happened before they even knew why; and third, before choosing from a “bad” deck, a polygraph (lie detector) machine detected a rise in their nervousness.
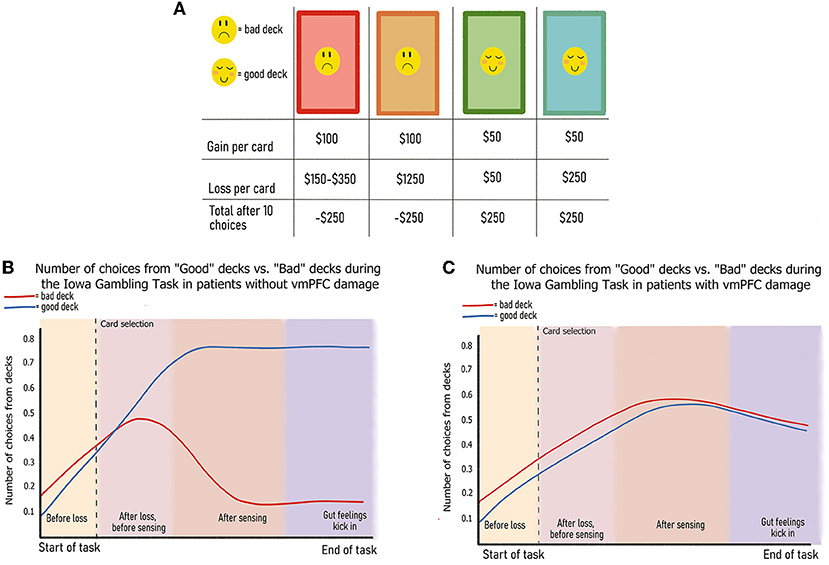
- Figure 2 - (A) Wins and losses associated with each deck of the Iowa Gambling Task (IGT).
- (B) Participants without vmPFC damage learn that “good” decks have larger rewards and choose more cards from “good” decks as the IGT goes on. (C) Participants with vmPFC damage do not learn that “good” decks have larger rewards and choose the same number of cards from “good” and “bad” decks as the IGT goes on.
When people with vmPFC damage played the IGT, they did not learn to avoid the “bad” decks—they continued to choose them and ended up losing all their money. Although patients with vmPFC damage can understand the game, there is a disconnect between what they know and what they do. In addition, people with vmPFC damage do not show increased nervousness before making “bad deck” choices the way healthy people do. They are unable to develop a “gut feeling” about the “bad” decks. As such, they continue to select from those decks because of the big wins, without being affected by their even bigger losses. These findings tell us that the vmPFC is important for combining knowledge with emotion in decision-making [1—3]. Specifically, the vmPFC plays a key role in developing “gut feelings” to guide favorable behaviors. These results led to the creation of the somatic marker hypothesis.
The Somatic Marker Hypothesis
The somatic marker hypothesis [1, 4] is a theory to help understand the unique behavioral changes Phineas Gage showed, and to make sense of how the brain, body, and emotions interact. The word “soma” comes from the Greek word for “body,” so somatic markers are the body’s way of signaling emotions. Somatic markers are situational, meaning the environments we are in help us decide whether we are feeling “good” or “bad” emotions. They are the body’s way of marking events with bodily signals/emotions to guide our behaviors [1, 4]. For example, getting butterflies in your stomach can indicate “good” emotions when you experience them with excitement, but they can also indicate “bad” emotions when something bad might happen.
Over time, we learn that certain bodily sensations, paired with emotions, can lead to specific outcomes [4]. For example, a terrifying encounter with your neighbor’s dog will make your heart pound, your limbs feel weak, your mouth dry, and your body shake with fear! You may feel these bodily sensations again when you think about cutting across your neighbor’s yard to get home sooner. These somatic markers act like a “spidey-sense” guiding your behavior—they make you feel that a shortcut through your neighbor’s yard is a bad idea, and help you choose a safer way home, so that you can avoid re-experiencing this fearful situation.
How Do Somatic Markers Influence Our Choices?
Somatic markers are bodily signals arising from the situations we are in, but how does the brain know what to do with them? The central nervous system, which is made up of the brain and spinal cord, takes information from the world and sends it to certain brain areas, including the thalamus, the vmPFC, and the amygdala. The thalamus detects sensations arising from somatic markers; the vmPFC links bodily signals with emotions; and the amygdala allows us to learn from our actions, to label situations as “good” or “bad,” and to know what to do the next time we are in a similar situation. The vmPFC ties everything together to guide our behaviors (Figure 3).
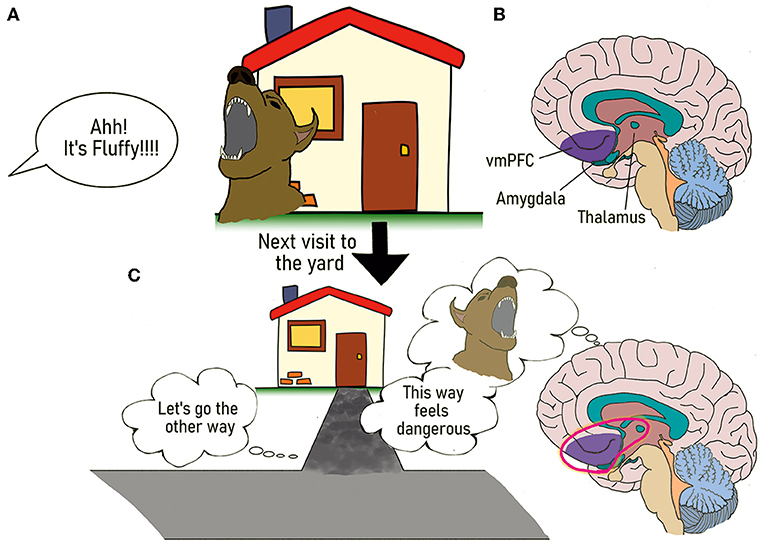
- Figure 3 - The somatic marker hypothesis.
- (A) First encounter with the neighbor’s angry dog when you decide to take a shortcut home. (B) Locations of the vmPFC, thalamus, and amygdala. (C) The memory of your neighbor’s mean dog comes into your mind the next time you have the option to cut through your neighbor’s yard to go home. Your vmPFC, thalamus, and amygdala work together to make you re-live feelings from your first encounter. To avoid facing your neighbor’s dog and re-experiencing feelings of fear, you decide to take a longer, safer way home.
For example, as you and your friend walk home together after school, your friend decides to cut through your neighbor’s yard to save time. Your thalamus recognizes the bodily sensations you experienced from a previous bad encounter with your neighbor’s dog (pounding heart, sweating, and dry mouth). The memory of this event, stored in your amygdala, warns you this is not a good idea. Your vmPFC links your previous emotions to your current experience and marks one option as more favorable than the other (taking the long way home is safe and not stressful). As such, you decide that it is best to take the long way home, and you convince your friend that it is the safer choice. Alternatively, as we saw with the IGT, people with vmPFC damage do not have the body signals alerting them about risky choices. Therefore, they have difficulty making good decisions when they only consider immediate rewards (like shortcuts) and not the penalties—even if they know there is a risk, they do not feel it. In this way, they continue to make bad decisions, because they have no somatic markers or “spidey-sense” guiding their choices.
Conclusion
Phineas Gage helped show us how important the vmPFC is for making good decisions—when the vmPFC is damaged, people have a hard time making good decisions. They have trouble planning their daily lives, thinking about the future, choosing good friends, and participating in social activities. Scientists believe that the inability to use emotions to help guide our behaviors explains why people who have vmPFC damage have problems with decision-making. Knowing how the vmPFC connects information from our surroundings with our feelings and our bodily responses to emotions, we can understand that damage to this brain area changes how we experience and interact with the world. It turns out that our built-in “spidey-sense,” combining body signals across multiple brain areas, helps us make good decisions.
Glossary
Ventromedial Prefrontal Cortex (vmPFC): ↑ A region of the brain located behind the eye sockets that plays an important role in decision-making.
Iowa Gambling Task (IGT): ↑ A research task that assess risky decision-making by involving the vmPFC.
Somatic Markers: ↑ Bodily responses signaling various emotions.
Thalamus: ↑ Found in the middle of the brain, the thalamus plays an important role in relaying sensory information from the body to other areas of the brain.
Amygdala: ↑ A brain region responsible for processing and detecting fearful and threatening stimuli, and plays an important role in emotional memory.
Acknowledgments
Illustrations were kindly provided by Kriti Manuja. The authors recognize and acknowledge that the land on which this work was completed is the traditional territory of the Mississauga and Haudenosaunee nations, and within the lands protected by the Dish with One Spoon wampum agreement.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
[1] ↑ Damasio, A. R. 1994. Descartes’ Error: Emotion, Reason, and the Human Brain. New York, NY: G.P. Putnam..
[2] ↑ Bechara, A., Damasio, A. R., Damasio, H., and Anderson, S. W. 1994. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50:7–15. doi: 10.1016/0010-0277(94)90018-3
[3] ↑ Bechara, A., Damasio, H., and Damasio, A. R. 2000. Emotion, decision making and the orbitofrontal cortex. Cereb. Cortex 10:295–307. doi: 10.1093/cercor/10.3.295
[4] ↑ Damasio, A. R. 1996. The somatic marker hypothesis and the possible functions of the prefrontal cortex. Phil. Trans. R. Soc. Lond. B 351:1413–20. doi: 10.1098/rstb.1996.0125