Abstract
Walking is an activity you do every day without even thinking about it. But have you ever wondered how we walk or why some people walk a bit strangely? We all limp when we hit a toe against the table or when we sprain a foot. But some people seem to walk even more strangely. Having difficulties with walking is not always the result of weak legs or a painful foot; some people walk differently because of trunk impairments. Besides having strong legs, it is important to have a stable trunk during walking to keep balanced. For instance, most people who have had strokes have problems with their legs and trunk, resulting in clear walking impairments. In this article, we explain how the trunk moves during walking in stroke survivors, and whether the observed walking impairments result from an unstable trunk or weakness in the legs.
Did you know that there are over 30 synonyms in the English language to describe walking? You can take a hike, step, stroll, or march. Some people seem to limp, hobble, stagger, lurch, or even waddle. A lot of words, right? Do not worry, all these words just describe that some people walk a little differently. Maybe your grandparents already walk a bit strangely and you do not know why. Many people think that abnormal walking patterns are a result of problems with the legs. This might be true in some cases, but not always. Sometimes people walk differently because they cannot control their trunk [1, 2].
What Exactly is the Trunk?
The trunk, or torso, is the central part of the body to which the arms, legs, and head are attached (Figure 1). The trunk consists of four parts: the shoulders, chest, belly, and pelvis. Most of the time we divide the trunk into an upper part, the shoulders and the chest, and a lower part, the belly and pelvis. Everything above the belly button is called the upper trunk and below, the lower trunk. The ability to control your trunk determines how well you can sit upright without falling or how well you can move your upper or lower trunk independently. Movements in the upper and lower trunk can be divided in three categories: (1) bending forwards or backwards; (2) bending left or right; and (3) turning to the left or right.
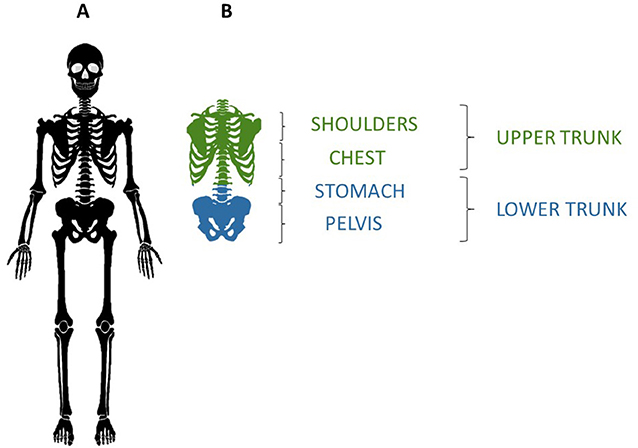
- Figure 1 - (A) The human skeleton.
- (B) The trunk can be divided into the upper trunk, which contains the shoulders and chest, and the lower trunk, which contains the stomach and pelvis.
In the early days when researchers were investigating walking, they thought that the trunk did not actively contribute to gait, which is the way a person walks [3]. They believed the torso was a passive part of the body and that the legs did all the work during walking. In more recent research, it has been determined that the trunk plays a much bigger role than researchers originally expected. For example, when comparing children with gait problems to healthy children, they found that incorrect trunk movements were one of the most important reasons why walking was so exhausting [4]. So, the ability to control your trunk and move it correctly in your gait is critical for walking efficiently.
Why Can’t Some People Control Their Trunk?
Some people who have suffered a stroke are unable to control their trunk. A stroke is a type of brain injury in which some brain cells die because of lack of oxygen, resulting from a blockage of the blood supply to the brain or bleeding in the brain. Blood vessels can become narrower as people age due to fat building-up in the blood vessel walls as a result of cigarette smoking, obesity, and lack of exercise, all of which increase the risk of stroke. Elderly people have the highest risk of suffering a stroke—more than 70% of all strokes occur in people over 65. But what does the brain do? Well, it acts like the conductor of an orchestra in which the musicians are the body’s muscles. Without a conductor for the musicians, there is musical chaos. Similarly, the brain tells the muscles what to do and when to do it, so we can move our bodies in harmony. When a part of the brain stops working because it did not receive oxygen, it stops guiding and instructing the muscles. Damaged brain cells are unrepairable, so other parts of the brain must learn how to take over the functions of these dead cells. That is why recovery after a stroke is long—the brain needs to relearn all these movements.
So, this is what happens to the muscles of the trunk, the back, and the belly of stroke survivors. The brain no longer gives those muscles good instructions, so the movements of the trunk are no longer performed correctly. Researchers have known for quite some time that stroke survivors have trunk problems and often cannot sit without the support of the hands and cannot roll around easily in their beds [5]. As we mentioned, the trunk is also important during walking. But to our surprise, we found that there was very little research about the movements of the trunk during walking in stroke survivors who have low trunk control. We made it our mission to find out more!
Measuring Trunk Movements and Walking Patterns
We studied 57 stroke survivors (39 males and 19 females) and 57 healthy individuals (35 males and 22 females). The age range in both groups was 19–85 years, with a mean age of 64 years. We assessed the strength and mobility of the trunk and legs of stroke survivors and categorized them into two groups: severe problems in the legs or no problems in the legs. In our gait laboratory, we examined both the stroke survivors and the healthy individuals. We measured all the movements of the body during walking with multiple cameras and used the information to create a 3D image. This is known as 3D motion analysis. Four force plates were used to provide information on when the feet contacted the ground1. We placed 39 reflective markers on each participant’s body, so that we could calculate how far and how much every part of the body was moving (Figure 2A). For the arms, markers were placed on each shoulder and elbow, two on each wrist, and one on each index finger. For the legs, one on each thigh, one on each knee, one on each shank, and three on each foot (ankle, heel, and toe). Four markers were also placed on the head, two on the chest, two on the back, and four on the pelvis. For a detailed analysis of the spine, four markers were placed on the upper trunk and three on the lower trunk.
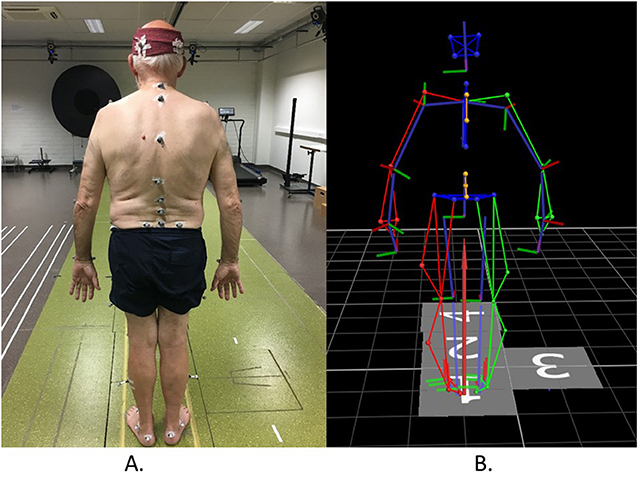
- Figure 2 - (A) The placement of reflective markers on the body of a study participant.
- Cameras placed around the lab emitted infrared light, which bounced off the reflectors and back to the cameras as the participant walked. (B) Each dot in the computer-generated image represents a reflective marker. The computer program connects the dots with colored lines (green = right arm and leg, red = left arm and leg, blue = trunk and head, orange = spine). The gray numbered squares are the force plates that measured each step. The red arrow shows the force measured by the force plates.
After attaching the markers, participants were asked to walk up and down a walkway a few times. The cameras, which were placed all over the laboratory, recorded the markers using infrared light. The cameras send out the infrared light, which bounces off the reflective markers and back to the cameras. From the information received by the cameras, we were able to make a 3D model of our participant using a computer (Figure 2B).
Using the 3D images, we then assessed the movements of the trunk, focusing on the three movements that were mentioned earlier: bending forwards or backwards, bending sideways, and turning to the left or right. We compared the degree of movement of the trunk in stroke survivors to that of healthy adults. Then, we compared trunk movements between stroke survivors with severe leg problems to stroke survivors with no leg problems.
Trunk Control is Critical for Walking!
The first research question, “How does the trunk move during walking in stroke survivors?” was investigated. We found that stroke survivors walk with shorter and wider steps and walk much more slowly compared to healthy adults. When looking at the trunk, we saw that stroke survivors also bent more forward as they walked and showed decreased rotations of the torso. This bent-forward position is also the reason that stroke survivors often cannot hold their bodies upright when sitting. In addition, stroke survivors could not turn the upper trunk to the right while turning their lower trunk to the left. This one is difficult to understand, right? Well, let us try it ourselves! Get up from you chair and find a place with lots of room to walk in a straight line, such as a hallway. Now walk very quickly, but do not run.
Did you notice that, when you took a step with your left foot, your right arm moved forward? And when you stepped with your right foot, your left arm moved forward? This is called cross-coordination. Although it is difficult to see, your upper and lower trunk do the same thing during walking: when your upper trunk turns right, your lower trunk turns left. These rotations are missing in stroke survivors—they walk without cross-coordination of the trunk, which is necessary for an efficient walking pattern. These rotations of the trunk are not generated by big strong muscles. Instead, they are created by accurately activating a specific muscle at a specific moment, so learning to control those muscles is key2.
Subsequently, we examined our second research question, “Is the trunk really the reason stroke survivors walk strangely?” We answered this by dividing the stroke survivors into two groups, people with and without severe problems in the legs. We found that people with more severe problems in the legs have more abnormal movements in the trunk. On the other hand, people with no severe problems in the legs also had some (but less) abnormal movements in the trunk. This means that even stroke survivors who do not have big problems with their legs still walk differently than healthy adults. However, it is very important to understand that you do not need extremely strong belly and back muscles to walk correctly. Proper walking is more about how well you can control and activate those muscles.
Why is Understanding Gait Problems Important?
Understanding why stroke survivors walk strangely can help researchers and doctors to help these patients recover. Stroke survivors need lots of therapy to get better. If doctors and physical therapists have a good understanding of whether the cause of a patient’s gait problems stems from the legs vs. the trunk, they can give the patients exercises that are focused on the specific problem—either strengthening the legs or improving trunk control. The results of our research showed that stroke survivors have abnormal trunk movements during walking, which in some cases are caused by lack of trunk control. So, giving these people exercises to help them learn to control their trunk, called core-stability exercises, might eventually help them walk better. Walking is an activity that contributes to a person’s independence and quality of life, so hopefully our research will eventually improve the lives of many stroke survivors.
Glossary
Trunk: ↑ The central part of the body, to which the arms, legs, and head are attached. Also called the torso.
Gait: ↑ A person’s way of walking.
3D Motion Analysis: ↑ A three-dimensional movement analysis where high technological instrumentation is used to assess movements of the human body.
Cross-coordination: ↑ The upper and lower part of the trunk moves in a coordinated, yet opposite manner. When the upper trunk rotates to the right, the lower trunk moves with a similar amplitude to the left.
Core Stability Exercises: ↑ Exercises focusing on strengthening back and belly muscles (a person’s core) and increasing the ability to control the position of the trunk.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
1. ↑ A virtual tour of the gait laboratory can be seen here (https://www.youtube.com/watch?v=QaEuXNA8fOA&feature=youtu.be)
2. ↑ Interested how this looks like in the 3D model measured by the Vicon motion analysis system, take a look at the videos here (https://www.youtube.com/watch?v=QaEuXNA8fOA&feature=youtu.be).
Original Source Article
↑Van Criekinge, T., Saeys,W., Herssens, N., Van deWalle, P., De Hertogh, W., Truijen, S., et al. 2020. Trunk biomechanics during walking after sub-acute stroke and its relation to lower limb impairments. Clin. Biomech. 75:105013. doi: 10.1016/j.clinbiomech.2020.105013
References
[1] ↑ Kavanagh, J. J., Barrett, R. S., and Morrison, S. 2005. Age-related differences in head and trunk coordination during walking. Hum. Mov. Sci. 24:574–87. doi: 10.1016/j.humov.2005.07.003
[2] ↑ Lamoth, C. J., Meijer, O. G., Daffertshofer, A., Wuisman, P. I., and Beek, P. J. 2006. Effects of chronic low back pain on trunk coordination and back muscle activity during walking: changes in motor control. Eur. Spine J. 15:23–40. doi: 10.1007/s00586-004-0825-y
[3] ↑ Murray, M. P., Drought, A. B., and Kory, R. C. 1964. Walking patterns of normal men. J. Bone Joint Surg. Am. 46:335–60.
[4] ↑ Van de Walle, P., Hallemans, A., Truijen, S., Gosselink, R., Heyrman, L., Molenaers, G., et al. 2012. Increased mechanical cost of walking in children with diplegia: the role of the passenger unit cannot be neglected. Res. Dev. Disabil. 33:1996–2003. doi: 10.1016/j.ridd.2012.05.029
[5] ↑ Verheyden, G., Nieuwboer, A., Feys, H., Thijs, V., Vaes, K., and De Weerdt, W. 2005. Discriminant ability of the Trunk Impairment Scale: a comparison between stroke patients and healthy individuals. Disabil. Rehabil. 27:1023–8. doi: 10.1080/09638280500052872