
Introduction
You can perceive things by touching, tasting, smelling, listening, and seeing. The sensory system that allows us to “feel” is called somatosensation (so-MAT-o-sen-sa-shun). Somatosensation is a broadly defined perceptual system that involves, among others, the experience of being touched or stroked on the skin, but also sensing temperature and feeling pain. In addition, somatosensation is responsible for registering the inside of the body. This system allows us to know where our body parts, e.g., your hands or feet, are located in space and is called proprioception (pro-pre-o-CEP-shun). The latter is crucial for programing our motor behavior. We need to know, even in the absence of visual feedback, where our body and limbs are in order to perform the correct movements. Finally, we can recognize objects by tactile exploration. Just think of trying to identify the contents of your pockets by feeling them, or to open a door with the correct key in the dark.
Given this spectrum of functions, it is not surprising that somatosensation is sub-served by a complex system entailing (i) a number of separate sensory organs in the skin, muscles, and joints; (ii) an extensive network of peripheral nerves connecting these sensory organs to the brain; and (iii) a constellation of brain structures to process all this information. Here, we will describe the most important aspects of somatosensation.
Peripheral Somatosensory Organs
Generally, each somatosensory sub-modality (e.g., touch, proprioception, sensitivity to hot and cold, and pain) is associated with different types of receptors (see Figure 1).
- Figure 1 - Examples of somatosensory sub-modalities.
Touch
There are various types of mechanoreceptors (receptors concerned with touch). In the hairy skin, the hair follicle receptor is the main mechanoreceptor. In addition, the hairy skin contains fibers that respond well to slow stroking with a soft brush, and stimulation of these fibers results in an experience of pleasant touch. The non-hairy skin contains four main types of mechanoreceptors, which can be divided into two functional groups. The first group contains fast adapting mechanoreceptors, which respond only at onset, and frequently at the end, of a touch, but not in between. The second group consists of slowly adapting mechanoreceptors, which respond slowly to the onset of a touch, but continue to respond during the middle. The density of mechanoreceptors varies in different parts of the body. Within the hand, the highest density of receptors is found in the fingertips. The higher the density of mechanoreceptors, the smaller the distance between two touches that can be distinguished.
Proprioception
Receptors in three different organs, skin, muscles, and joints, can contribute to proprioception. In the skin, slowly adapting receptors respond to lateral stretching of the skin. Two main types of receptors can be found in muscles, muscle spindles and golgi tendon organs. Golgi tendon organs are situated at the junction between muscles and tendons. Joint receptors are similar to those found in the skin and muscle.
Hot/Cold receptors
Two types of specific cutaneous thermoreceptors, which cannot be easily excited by non-thermal stimuli, have been found. Cold receptors are excited by a drop in skin temperature but stop firing when the skin temperature rises. Warm receptors respond in an opposite manner, i.e., they increase firing when the skin temperature rises but become silent when the temperature decreases.
The main processing pathways of the somatosensory system, from peripheral receptors to the cortex, which are concerned with touch and proprioception are well known. Input from peripheral receptors ascends through the dorsal (toward the back) column in the spinal cord and subsequently arrives in the medulla (part of the brain). The fibers then cross over (blue line in Figure 2), from left to right, and vice versa, in the medial lemniscus, and terminate in the thalamus, in the ventral posterior lateral nucleus to be precise. A second ascending system, the anterolateral (to the front and at the side) system, mainly deals with thermal and noxious stimuli but also relays some pressure information. The anterolateral system also projects to the thalamus, again the ventral posterior lateral nucleus, and to a few smaller nuclei. It also crosses over earlier within the spinal cord (orange line in Figure 2).
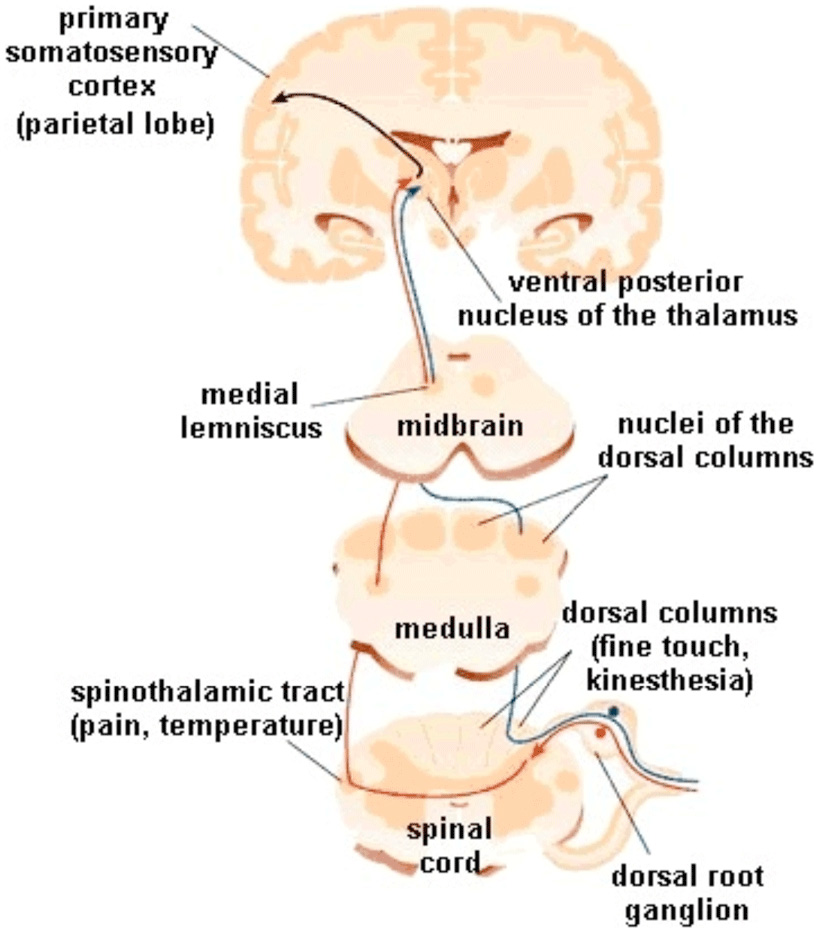
- Figure 2 - Somatosensory pathways from the spinal cord to the somatosensory cortex.
Feature Processing in the Primary Somatosensory Cortex
Most somatosensory information enters the cerebral cortex through projections from the thalamus to the anterior parietal cortex. This area is known as the primary somatosensory cortex (SI) (see Figure 3 left). In fact, the SI consists of number of different areas (called Brodmann areas 1, 2, 3a, 3b) that all receive separate inputs from the thalamus. These four different areas all contain somatotopic maps of the contralateral half of the body. Somatotopic means that different parts of the body are separately represented over the surface of the cortex. However, the amount of cortical surface is not always proportional to the size of the body part. Rather, the most sensitive body areas, such as the hands and lips, occupy a larger part of SI (see Figure 3 right).
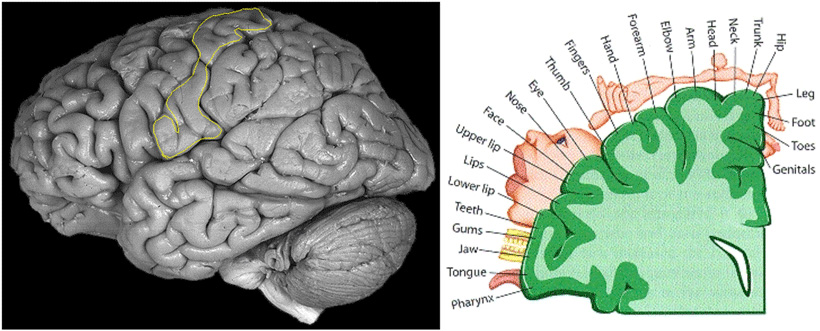
- Figure 3 - The primary somatosensory cortex (SI).
It is interesting to note that one somatosensory aspect tends to dominate the input to each area, i.e., the different areas in SI appear to be specialized for a specific aspect of the somatosensory input. For instance, in areas 3a, the dominant input originates in the muscle receptors, and in areas 3b and 1, the main input originates in skin receptors. Within these Brodmann areas, specific regions are activated by different types of stimulation such as vibration or pressure.
In the early stages of cortical processing, the neuronal activity represents the characteristics of stimuli applied to peripheral nerves relatively accurately. Neurons situated further away from the thalamic input have more complex response properties, suggesting that advanced processing occurs. For example, neurons that register the direction of a movement over the skin are not very common in the first port of call, i.e., area 3b, but much more common in the subsequent areas 1 and 2.
At this point, it is important to discuss a clinical phenomenon that provides us with a unique insight into the brain. Some patients who can no longer consciously tell where they were touched, for instance, their arm, may still be able to accurately point to the stimulated position. In a now classic study [1], Volpe et al. [1] reported four patients with tactile and proprioceptive deficits after a stroke who could not feel where their arm was, but who were nevertheless able to perform spatially oriented movements with the deafferented hand. It seems that the information about the spatial position of the arm that was no longer consciously accessible to the patient was still present at an unconscious level and used by the motor programing for the pointing action. This phenomenon was called “numbsense,” and it is strikingly similar to “blindsight” where patients may still be able to point to stimuli presented in their blind visual field. It thus appears that somatosensory information can be used for the guidance of movements after lesions to the primary somatosensory cortex. It is proposed that this phenomenon, that is poorly understood, depends on thalamic projections to the posterior parietal cortex. Bypassing the anterior parietal cortex may therefore be responsible.
Higher Somatosensory Cortical Processing
Processing of somatosensory input beyond the anterior parietal cortex occurs in several cortical areas. They include secondary somatosensory area (SII), the insula (Figure 4 right), and the posterior parietal cortex (Figure 4 left). An obvious question is what are the roles of these three strongly interconnected areas. A good way to start is to look at what we use somatosensory information for, as follows.
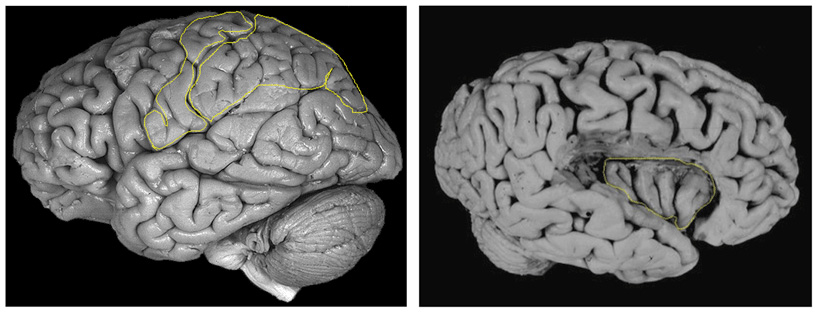
- Figure 4 - The secondary somatosensory area (SII).
Tactile Exploration
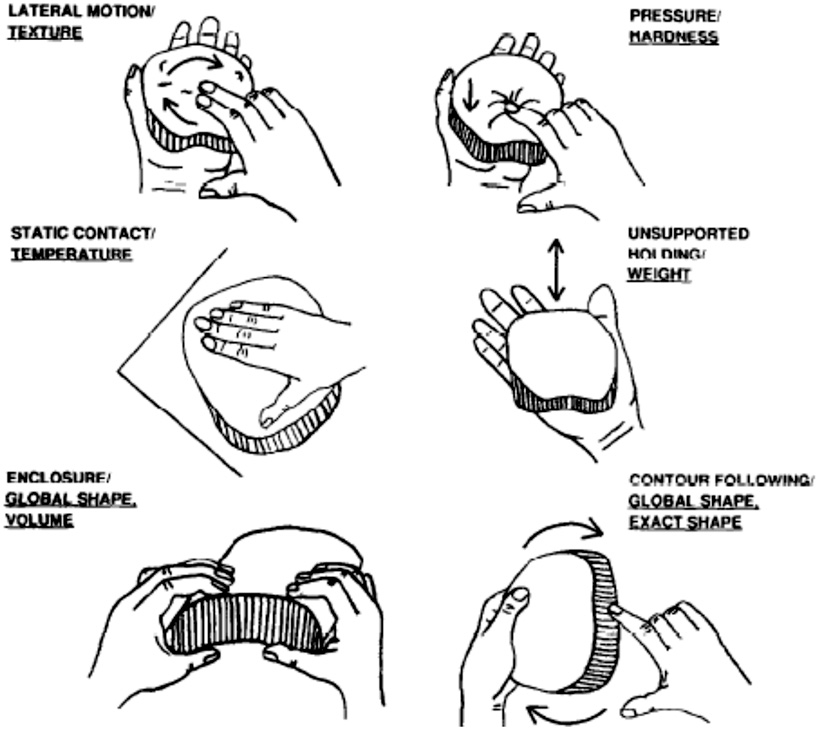
One major function of the somatosensory system is the recognition of external stimuli, such as objects. We frequently make use of tactile perception to recognize objects in our daily lives, for example, when retrieving our keys from our pants pocket. Recognizing objects by touch is usually not a passive process. The stimulus is typically explored actively using finger and hand movements to build an internal object representation. These finger and hand movements are not random but depend on the object characteristics that need to be identified. When people are asked to discriminate a particular object’s dimensions or characteristics (e.g., texture, hardness, weight), different types of hand movements or routines, named exploratory procedures, are used. For example, texture was mainly explored through sideway movements between skin and object surface (lateral motion) (see Figure 1).
When identifying objects, sequences of exploratory procedures are performed that together help to build an internal representation that can be matched with object representations in memory.
Cortical Processing of Somatosensory Information Pertaining the Body
Perhaps an even more important function of the somatosensory system is informing us about the position of our different body parts with respect to each other. To achieve this, tactile and proprioceptive input needs to be integrated with visual and vestibular input into a representation of the body. Moreover, stored knowledge about our body plays an important role.
Thus, we use tactile information in two important ways. We suggested [2] that the system responsible for somatosensory processing, for the immediate guidance of action, is subserved by a route that runs from the primary somatosensory area, anterior parietal cortex, either directly or via the SII, to the posterior parietal cortex. This area is subsequently involved in cross-modal integration and the preparation of movements. The processing of somatosensory processing for conscious perception and memory is performed by a system that culminates in the insula. In addition, the right posterior parietal cortex appears to be involved in spatiotemporal integration of somatosensory input during recognition of objects and body configurations, while the left posterior parietal cortex has been implicated in structural and semantic body representations.
By now, it will be clear that “feeling” is a very complicated human ability. We have a number of specific receptors in our skin and body, the signals they pick up are transferred to the brain via a number of pathways. In the brain, a number of different areas or structures process specific aspects of the incoming somatosensory information. Finally, this information is used to feel, to recognize objects, and to make accurate movements. It will also be clear from this review that if things go wrong, like in patients with brain damage, people may suffer very specific and incapacitating impairments. It is important that we gain an in-depth understanding of the somatosensory system in order to help these patients.
References and Further Reading
The famous case description of the patients with numbsense was published in:
[1] ↑ Volpe, B. T., LeDoux, J. E., and Gazzaniga, M. S. 1979. Spatially oriented movements in the absence of proprioception. Neurology 29:1309–13. doi: 10.1212/WNL.29.9_Part_1.1309
There are a large number of articles and books that we have used for this review but we will not bore you with a list of references. Most of the original sources we used can be found in our paper:
[2] ↑ Dijkerman, H. C., and de Haan, E. H. 2007. Somatosensory processes subserving perception and action. Behav. Brain Sci. 30:139–89. doi: 10.1017/S0140525X07001641
Two instructive book chapters are:
Gardner, E. P., Martin, J. H., and Jessell, T. 2000. The bodily senses. In Principles of Neural Science, 4th Edn, eds. E. R. Kandel, J. H. Schwartz, and T. M. Jessell, 430–50. New York: McGraw-Hill.
Mountcastle, V. B. 1984. Central mechanisms in mechanoreceptive sensibility. In Handbook of Physiology, Section 1: The Nervous System, vol. III, ed. J. M. Brookhart, 789–878. Bethesda: American Physiological Society.
A lot of our ideas are based on the work of:
Paillard, J. 1999. Body schema and body image – a double dissociation in deafferented patients. In Motor Control, Today And Tomorrow, eds. G. N. Gantchev, S. Mori, and J. Massion, 198–214. Bulgaria: Academic Publishing House.
Milner, A. D., and Goodale, M. A. 1995. The Visual Brain In Action. Oxford: Oxford University Press.