
Abstract
Primary progressive aphasia (PPA) is a rare disorder that affects older adults, causing them to slowly lose the ability to communicate. PPA is caused by certain diseases that damage brain cells in areas of the brain that control speech and language. There are three types of PPA, each with unique speech and language symptoms. While there is not currently a “cure” for the diseases that cause PPA, there are a number of ways to support communication and promote quality of life for individuals with PPA, for as long as possible.
Introduction
As we age, there are ways we continue to grow. For example, the older we get, the more we learn about the world and the more our vocabularies grow. It is also normal to find some tasks more difficult, such as hearing what someone is saying in a crowded place. However, certain health conditions can alter the abilities of older adults beyond the changes we expect to see with normal aging. In this article, we will focus on one of these conditions: primary progressive aphasia, or PPA.
What is Primary Progressive Aphasia?
Neurons are brain cells that control everything we do. They play an important role in thinking, talking, and all of our daily activities. Neurons are somewhat specialized—certain groups of neurons are responsible for specific tasks. If neurons in areas of the brain that control language are damaged, this will lead to aphasia. People with aphasia struggle to produce and/or understand language. Brain damage may result from several causes, but stroke is the most common cause of aphasia. During a stroke, part of the brain does not receive enough blood and the neurons in that area are damaged or may die (to learn more about aphasia caused by stroke, read this Frontiers for Young Minds article). Aphasia can also be caused by neurodegenerative diseases, which are diseases that damage neurons in the brain over time, increasingly affecting a person’s brain functions. The location and extent of neuron damage determine the symptoms or changes in abilities that a person will experience.
When aphasia is caused by neurodegenerative disease, it is called primary progressive aphasia (PPA) [1]. PPA damages neurons in brain areas related to speech and language, making it harder and harder to communicate. With time and speech-language therapy, people who have aphasia due to stroke sometimes recover their speech and language skills. However, for people with PPA, speech and language problems inevitably worsen over time. There is no known drug proven to cure PPA or stop PPA from getting worse. Eventually, the disease starts to affect areas of the brain outside speech and language regions, causing difficulties with other functions like problem solving, movement, or swallowing.
To understand how PPA affects a person’s brain, scientists and doctors often use a brain-imaging technique called magnetic resonance imaging (MRI; Figure 1). Because scientists have mapped the areas of the brain that are responsible for specific functions, it is possible to look at an MRI scan and predict what kinds of difficulties a person may experience based on patterns of damage.
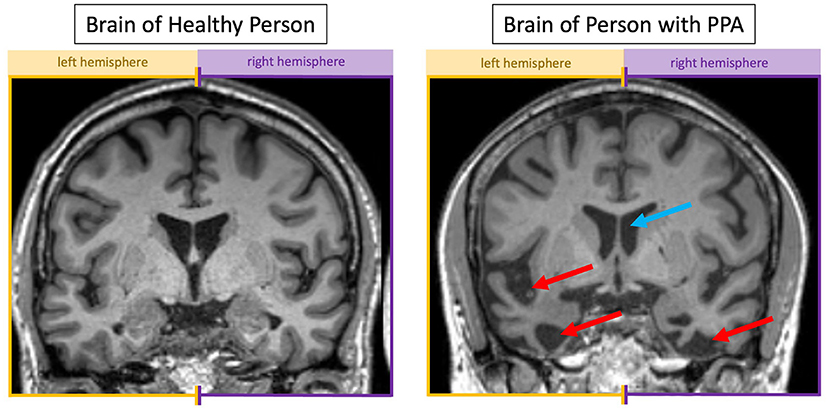
- Figure 1 - An MRI scan of (left) a healthy older adult and (right) someone with semantic PPA.
- Looking at someone face-to-face, this brain “slice” is halfway between their face and back of their head. Where neurons have died, there is more dark space. The blue arrow is pointing to a fluid-filled space that we expect to show up as dark. The red arrows show larger dark spaces indicative of brain shrinkage resulting from dying neurons. The left side of the PPA brain has more dark spaces than the right, which is expected since the left side of the brain generally controls language.
The Three Types of PPA
There are three types of PPA, each with its own pattern of symptoms: semantic, logopenic, and nonfluent/agrammatic [2]. All people with PPA have difficulties with speech or language; however, damage to different areas within the brain’s speech-language network results in distinct speech and language symptoms.
People with the semantic type of PPA gradually lose semantic memory—memory for facts about the world, like who is the president, that a squirrel is a small mammal, or that fire is hot (semantic memory is explained further in this Frontiers for Young Minds article). For example, someone with semantic PPA might see a boy crying and say that he “has water in his eyes” because they cannot remember the word “tears” or they do not remember what tears are. Someone with semantic PPA might also have trouble following a conversation because they do not know the meaning of some of the words being said.
Logopenic PPA is characterized by difficulty with processing and assembling the sounds that make a word. Consider how the word “celebration” has several sounds in it (“s” “eh” “l” “uh” “b” and so on). Someone with logopenic PPA might have trouble putting the sounds together correctly and might substitute the wrong sounds (e.g., “sell-uh-gray-shun”) or put them in the wrong order (e.g., “bell-uh-stray-shun”). Similarly, individuals with logopenic PPA have difficulty processing speech sounds they hear. If they hear a long sentence, they might have trouble processing the words quickly enough to understand the sentence.
Lastly, people with the nonfluent/agrammatic type of PPA may struggle to produce and understand sentences and/or have trouble coordinating movements of the parts of the body used for speech, like the tongue, lips, and vocal folds. Someone with nonfluent/agrammatic PPA might be hard to understand, as their words might not sound quite right. If you have ever eaten something very cold that numbed your mouth, you might have noticed it was harder to move your tongue quickly when speaking, making your speech sound different. In the same way, if neurons controlling the movement of the tongue are damaged, a word might not sound like it is supposed to. Often, the speech of people with the nonfluent/agrammatic type of PPA contains long pauses and missing words. Typically, function words like “the” and “of” are left out. These function words do not mean much on their own but are essential for building grammatical sentences. For example, instead of saying “the boy is eating cake,” someone with nonfluent/agrammatic PPA may say “boy…eat…cake.”
The areas of the brain affected in each type of PPA are shown in Figure 2.
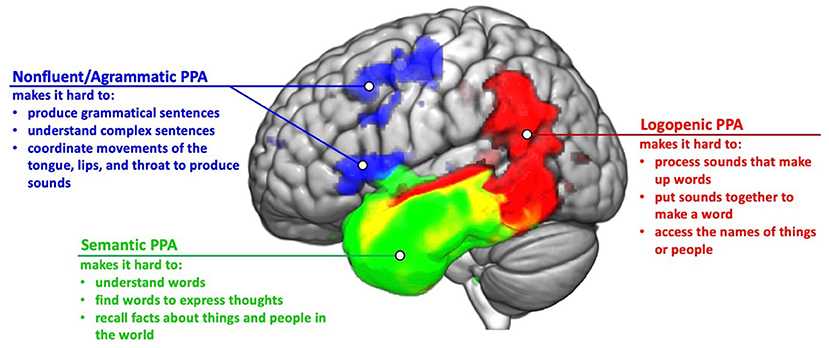
- Figure 2 - Damage to different brain areas results in the three types of PPA.
- Main symptoms for each type of PPA are summarized. In nonfluent/agrammatic PPA, the frontal lobe (at the front of the brain) is mainly affected. In semantic PPA, the temporal lobe (above the ears) is mainly affected. In logopenic PPA, the temporal and parietal lobes (near the back and top of the head) are mainly affected. The yellow area shows where damage can overlap in semantic and logopenic PPA.
How Can We Help People With PPA?
Although researchers have been working hard to find a cure, there is currently no medical treatment that can slow or reverse the effects of PPA. However, there are many ways speech-language therapists can help people with PPA to maximize communication and quality of life [3]. With therapy, people with PPA may be able to relearn lost skills and develop strategies to work around their communication difficulties. Research shows that some effects of therapy are short term whereas others can be longer lasting. In general, the goal of speech therapy is to make sure that people with PPA can participate in activities that are meaningful for them (e.g., talking with friends and family, ordering dinner at their favorite restaurant) for as long as possible.
In the earlier stages of PPA, speech therapy might focus on strategies for recalling particular words in conversation, or for making it easier for others to understand the words the person with PPA is trying to say. For example, a therapist can work with someone with PPA to develop scripts about topics they would like to discuss (e.g., football, hobbies, or their grandchildren), helping them practice so they can say the words clearly and form full sentences [4]. As PPA progresses and speaking gets more difficult, therapy might focus more on using alternative modes of communication like writing, gesturing, or using supportive communication devices. A communication tool might be a printed communication book, which can contain photos and names of important people, places, or objects that the person can refer to during conversation. Communication devices can also be higher tech, like speech-generating devices that can “speak” for the person with PPA. Speech therapists can also provide family members and loved ones with communication strategies to support the person with PPA.
Eventually, people with PPA might completely lose the ability to communicate verbally and may begin to have difficulties outside of speech and language, such as trouble with memory, walking, or swallowing. At this point, therapy might focus on people’s remaining skills and abilities, with the aim of helping each individual to continue with their daily activities and participate in their community to the fullest possible extent. This helps people with PPA retain a level of personal choice and a sense of self-worth.
There are many ways that people with PPA can continue to participate in life even if they struggle to communicate. People with PPA may continue their hobbies and creative pursuits, or sometimes even start new activities (e.g., painting, photography, woodworking) that help them to stay engaged. Ideally, they will remain socially active, spending time with friends and family who bring fulfillment. This may mean finding new ways to communicate and connect nonverbally as spoken communication becomes more challenging.
Conclusion
PPA is a condition that causes people to gradually lose their ability to communicate. People with PPA experience continued worsening of their symptoms because the disorder is caused by a neurodegenerative disease. There are three types of PPA that affect different aspects of speech and language. The semantic type affects a person’s knowledge about things and people. The logopenic type affects a person’s ability to process sounds that make up words. The nonfluent/agrammatic type affects the ability to produce and understand sentences and/or the ability to coordinate movements to produce speech. Researchers are working hard to find a cure for PPA. In the meantime, there are a number of treatment options that can improve communication and quality of life for these individuals for as long as possible.
Glossary
Neurons: ↑ Also called brain cells, neurons are the types of cells that make up the brain and spinal cord.
Aphasia: ↑ A language disorder, caused by damage to the brain, which can impact speaking and understanding language as well as reading and writing.
Stroke: ↑ When one of the blood vessels in the brain is blocked or bursts, preventing oxygen and nutrients from reaching part of the brain and causing damage.
Neurodegenerative Diseases: ↑ Diseases that affect the brain, slowly causing brain cells to die. There are many types of neurodegenerative diseases, and they have different symptoms and causes. One example is Alzheimer’s disease.
Speech-Language Therapy: ↑ Work with a speech therapist that addresses a variety of difficulties including trouble with language, speech, and swallowing.
Magnetic Resonance Imaging: ↑ An imaging method that lets us see inside the brain and other parts of the body using a large machine with a strong magnet.
Semantic Memory: ↑ Memory for facts about the world, like who the president is, what color an apple is, or how many continents there are on Earth.
Processing: ↑ In this article, processing refers to how the brain takes information from the external world, breaks it down, and manipulates it to understand and organize the information.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
[1] ↑ Mesulam, M. M. 2001. Primary progressive aphasia. Ann. Neurol. 49:425–32. doi: 10.1002/ana.91
[2] ↑ Gorno-Tempini, M. L., Hillis, A. E., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S. F., et al. 2011. Classification of primary progressive aphasia and its variants. Neurology 76:1006–14. doi: 10.1212/WNL.0b013e31821103e6
[3] ↑ Wauters, L. D., Croot, K., Dial, H. R., Duffy, J. R., Grasso, S. M., Kim, E., et al. 2023. Behavioral treatment for speech and language in primary progressive aphasia and primary progressive apraxia of speech: a systematic review. Neuropsychol. Rev. 1–42. doi: 10.1007/s11065-023-09607-1
[4] ↑ Henry, M. L., Hubbard, H. I., Grasso, S. M., Mandelli, M. L., Wilson, S. M., Sathishkumar, M. T., et al. 2018. Retraining speech production and fluency in non-fluent/agrammatic primary progressive aphasia. Brain 141:1799–814. doi: 10.1093/brain/awy101