Abstract
Have you ever felt “groggy” after hitting your head? We are learning more about how important it is to protect your brain from injuries, such as concussion. Concussion is also called mild traumatic brain injury (mTBI). After an mTBI, most people think patients recover within a few weeks. We noticed that some college students who had had an mTBI were struggling to remember information for a few seconds. This ability is called working memory and we need it for most thinking jobs, like remembering the name of someone you just met, or what you wanted to get from the fridge. In our experiments, we tested different groups of students to see if they could remember things for 1 s, like the color of squares. Participants with a history of mTBI (on average, more than 4 years after injury) performed worse than students without a history of mTBI. The take-home message is that there can be lasting effects of mTBI, even years after it happens.
What Happens After a Concussion?
Accidents happen all the time, due to falls, car accidents, and sports. Often, in accidents, people hit their heads. In the USA, mild traumatic brain injury (mTBI) results in >200,000 hospitalizations per year [1]. mTBI causes the brain to move, twist, or bounce against the inside of the skull. This can stretch and tear brain cells even though the brain is protected by a cushion of liquid called cerebrospinal fluid, several layers of tissue, and the skull. Some people even lose consciousness during an mTBI. People may not appear injured from the outside after an mTBI. Medical professionals have to diagnose an mTBI by physical examination and by asking questions. Soon after an mTBI, people often report symptoms including headaches, trouble with coordination and sleep, feeling slowed down (“mental fog”), difficulty concentrating, feeling emotional, and memory loss. A few weeks after an mTBI, symptoms usually go away and people slowly return to their daily activities, including school and sports.
Most research on mTBI includes people during the acute (0–7 days after injury) and subacute (up to 3 months after injury) stages of recovery. Only a little research studies what happens more than 3 months after injury. This is probably because of the assumption that everyone fully recovers. But there can be lasting problems with thinking, even years after an mTBI [2, 3]. This is an important point, because it means that some people do not fully recover after an mTBI.
Can MTBI Affect Brain Functions, Like Memory?
Executive functions are thinking abilities that allow us to achieve our goals. For example, executive functions allow you to stay on task, plan ahead, hold onto thoughts, solve problems, and refrain from inappropriate actions (like talking back to a teacher). In patients who had experienced TBI more than 4 years ago, we studied an executive function called working memory, which is the mental workspace that holds information for immediate use. For example, remembering the numbers the teacher writes on the board as you write down the problem in your notebook. Working memory differs from what is called long-term memory, which is what we use to remember events over years. For example, working memory helps us do addition in our heads, long-term memory is what allows us to remember our first day at school.
Working memory has three stages: encoding (putting information in), maintenance (holding on to that information), and retrieval (remembering that information and using it). Usually, people can hold about 3–5 things in working memory at a time. Working memory requires cooperation between regions in both the front and back of the brain. If brain cells in either of these regions are damaged, working memory could suffer. Although some researchers observed normal working memory shortly after mTBI [4], others saw that working memory is worse after mTBI, even years after injury [5, 6]. A problem in understanding the lasting effects of mTBI is that injuries vary, and everyone’s brain and recovery are different.
To study whether mTBI affects the executive function of working memory in patients who had mTBIs in the past we asked two questions. First, we asked whether college students with a history of mTBI performed differently on a working memory task compared with students without a history of mTBI. Second, we asked whether one of the stages of working memory—encoding, maintenance, or retrieval—was more hurt by the mTBI.
How Did We Test Our Questions?
To determine whether working memory was affected by mTBI, we tested students with a history of mTBI, averaging 4 years post-injury, and a control group that was made up of students who had no history of mTBI. Participants had to use working memory to remember the colors of squares that were briefly flashed on a computer screen. The experiment asked students to do a lot of trials that went as follows. First, student focused on the center of the screen, a cue appeared (white >), indicating where the student should attend (outlined in dashed box)—either the left or the right side of fixation. Then, after a short pause, 1, 2, or 3 colored squares quickly flashed on each side of the screen. On one side they were attending (and on the side they were ignoring) the colored squares. This image was the working memory encoding phase which allowed some of the colored squares to enter working memory. Next, there was a short pause, or maintenance period, during which the student tried to hold in working memory the color of each square. Finally, the retrieval stage was a test of working memory. One square appeared on the attended side of the monitor and the student pressed keys to indicate whether it matched or mismatched the color shown during encoding. An example of one trial of this task is shown in Figure 1, and participants did hundreds of trials.
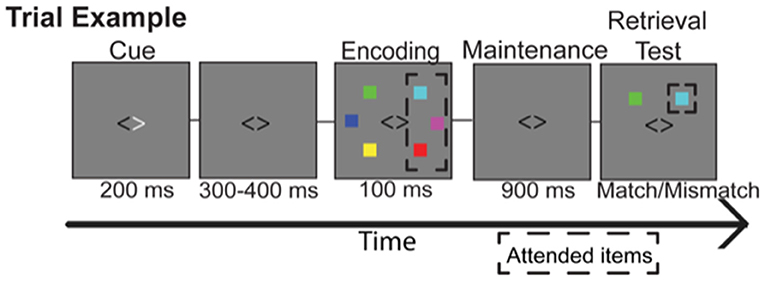
- Figure 1 - How did we test the three phases of working memory? Participants included students with a history of mTBI (averaging >4-years post-mTBI) and a control group, without a history of mTBI.
- The task was on a computer. Students kept their eyes on the center of the screen. First, a white cue (< or >) pointed to the side of the screen to attend to (dashed box indicates the attended items), while ignoring the squares on the other side. Then, colored squares flashed (100 milliseconds (ms), or 1/10 of a second). Students tried to encode (remember), the color of each square on the attended side. Next, during maintenance, students tried to remember each square’s color. Finally, there was a retrieval test. Students judged whether one colored square (inside the dashed square) matched the color shown during encoding.
Then, to see if one stage of working memory was more affected by mTBI than the others, we made each stage of working memory easier or harder. One way we did this was to change how long the stage lasted. For example, lengthening encoding by showing the squares longer makes it easier because there is more time to attend to the different colors. Even when we made the task easier the mTBI group still did worse. This told us that the problem is not with one particular stage of working memory. We think it is more likely that each stage is a little bit worse in the mTBI group.
What Did We Find and What Do Our Results Mean?
First, we found that, overall, students with a history of mTBI did worse on our working memory tasks than students without a history of mTBI (Figure 2). This is surprising because it was about 4 years since the students had had an mTBI and most people think that we get completely better after an mTBI. The results mean that there can be lasting changes after an mTBI. We found problems with working memory and we are now seeing problems with attention. We think there could be other problems, too, and we are now using more kinds of tasks to better understand what kinds of lasting changes are likely.
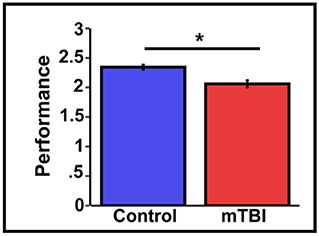
- Figure 2 - Students with a history of mTBI remember less than the control group.
- The control group (blue bar) remembered almost 2.5 (out of 3) colored squares, but the mTBI group (red bar) only remembered about 2. The * means this difference is statistically significant. We used mathematical tests to tell us if the difference between the two groups is more than would be expected by chance. We found that it did, so it is called significantly different. These results and others we performed told us that students with a history of mTBI are worn at working memory tasks.
When we asked whether one stage of working memory was more affected by mTBI, we found that the encoding, maintenance, and retrieval stages of working memory seemed to be equally affected. Even when we made each stage of working memory easier, we still saw that the mTBI group performed worse. For example, making encoding longer did not help the mTBI group, nor did making the maintenance duration shorter. We do not think that just one stage of working memory is causing the problem; instead, problems can happen at each stage of working memory. This will probably make it harder to fix because we need to work on improving encoding, maintenance and retrieval in the mTBI group to help improve working memory.
So, what does this mean for you? Take care of your head! Having an mTBI can hurt a person’s working memory for a long time, even years after the injury. Prevention is important because we do not know how to fix problems with thinking tasks, such as working memory. In our study, we learned that no single stage (encoding, maintenance, or retrieval) of working memory could explain the working memory problem in the mTBI group. We saw that college with a history of mTBI could not remember as many colored squares as students who did not have mTBI. This could mean that they have to study more to do well in their classes, and college is hard enough already. Preventing head injuries is important. Wearing a helmet protects you from head injuries today and protects you from the effects of mTBI months and years into the future.
Why is This Research Important?
This research is important because mTBIs should be taken seriously. Right now there is no blood test or brain scan that can reliably detect an mTBI. mTBIs require medical attention, and mTBI sufferers should follow the medical advice of their doctors. Brain injuries need time to heal and we need to learn more about how to help people recover. Researchers must continue to study what is happening to the brain after an mTBI. For example, our group wants to find out why some people with a history of mTBI do not show impairments in working memory. Maybe this information will help us to find ways to help those patients who do have working memory problems, so that all mTBI survivors can return to a normal working memory capacity.
Glossary
Mild Traumatic Brain Injury (mTBI): ↑ Also known as concussion, a condition of brain damage due to force applied to the head.
Executive Function: ↑ Abilities that allow us to get our work done. These abilities include paying attention, planning ahead, staying on task until it is done, and not doing something we know is not allowed.
Working Memory: ↑ The “mental workspace” that holds on to a few pieces of information for immediate use. It includes three stages: encoding (putting information in), maintenance (holding onto information), and retrieval (remembering what was put in).
Encoding: ↑ Putting something into working memory. For example, the colored squares are put into working memory during the encoding stage.
Maintenance: ↑ Holding on to information in working memory.
Retrieval: ↑ Remembering information that is in working memory. For example, knowing the color of the top squares after they disappear from the screen.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Original Source Article
↑Arciniega, H., Kilgore-Gomez, A., Harris, A., Peterson, D. J., McBride, J., Fox, E., et al. 2019. Visual working memory deficits in undergraduates with a history of mild traumatic brain injury. Atten. Percept. Psychophys. 81:2597–603. doi: 10.3758/s13414-019-01774-9
References
[1] ↑ Faul M, Xu L, Wald MM, Coronado VG. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Atlanta, GA: Centers for Disease Control and Prevention; National Center for Injury Prevention and Control (2010).
[2] ↑ Bajaj S, Dailey NS, Rosso IM, Rauch SL, Killgore WDS. Time-dependent differences in cortical measures and their associations with behavioral measures following mild traumatic brain injury. Hum Brain Mapp. (2018) 39:1886–97. doi: 10.1002/hbm.23951
[3] ↑ Dall’Acqua P, Johannes S, Mica L, Simmen HP, Glaab R, Fandino J, et al. Prefrontal cortical thickening after mild traumatic brain injury: a one-year magnetic resonance imaging study. J Neurotrauma. (2017) 34:3270–9. doi: 10.1089/neu.2017.5124
[4] ↑ Belanger HG, Curtiss G, Demery JA, Lebowitz BK, Vanderploeg RD. Factors moderating neuropsychological outcomes following mild traumatic brain injury: a meta-analysis. J Int Neuropsychol Soc. (2005) 11:215–27. doi: 10.1017/S1355617705050277
[5] ↑ Gosselin N, Bottari C, Chen JK, Huntgeburth SC, De Beaumont L, Petrides M, et al. Evaluating the cognitive consequences of mild traumatic brain injury and concussion by using electrophysiology. Neurosurgical Focus. (2012) 33: 1–7. doi: 10.3171/2012.10.FOCUS12253
[6] ↑ Hudac CM, Cortesa CS, Ledwidge PS, Molfese DL. History of concussion impacts electrophysiological correlates of working memory. Int J Psychophysiol. (2018) 132:135–44. doi: 10.1016/j.ijpsycho.2017.09.020