
Abstract
Scientists who study the brain try to understand how it performs everyday behaviors like language, memory, and emotion. Scientists learn a lot by studying how these behaviors change when the brain is damaged. Over the past 200 years, they have made many discoveries by studying individuals with brain damage. For example, one patient could not form sentences after damaging a specific area of his brain. The scientist who studied him concluded that the damaged brain area was important for producing speech. This approach is called the lesion method, and it has taught us a lot about the brain. In this article, we introduce five patients throughout history who forever changed our understanding of the brain. We describe how researchers use these early discoveries to ask new questions about the brain, and we conclude by discussing how the lesion method is used today.
Is there a place in the brain that helps us remember what we did in school yesterday or the names of people we meet? What about a place that helps us talk? Or a place in the brain that controls our personalities? If you have wondered about the answers to these questions, you are not alone! Scientists have searched for these answers for a long time. One way to find the answers is to study patients with brain damage. When an area of the brain is damaged, it is called a lesion. Scientists study patients who have lesions in specific parts of the brain. This helps them learn what the damaged part of the brain normally does. For example, what could that person do before their brain injury that they cannot do anymore? This method of studying the brain is called the lesion method. Scientists use the lesion method to understand the relationship between the brain and everyday behaviors. In this article, you will learn about five patients whose brain injuries forever changed them. You will see examples of how brain injury can change a person’s personality, ability to speak, memory, or sense of fear. You will discover how these people (and the scientists who studied them) changed how we think about the brain. Lastly, we will describe how the lesion method is used today. Scientists can combine the lesion method with other methods to make new, cutting-edge discoveries about the brain.
Patient 1: The Brain and Personality (1848)
What would it be like if your whole personality changed in an instant? Phineas Gage was a construction worker for a railroad company. As part of his job, he placed explosives to blow up rocks to clear a path for the railroad. Phineas dug holes, placed dynamite in them, then covered them with dirt. He used a metal rod called a tamping iron to pack the dirt. One day, Phineas was packing dirt over some dynamite. His iron grazed a rock, causing a spark. The dynamite exploded, rocketing the rod through Phineas’ skull. It entered his head under his left cheekbone and exited through the top of his skull (Figure 1). This destroyed a part of his brain located behind the forehead, called the frontal lobe.
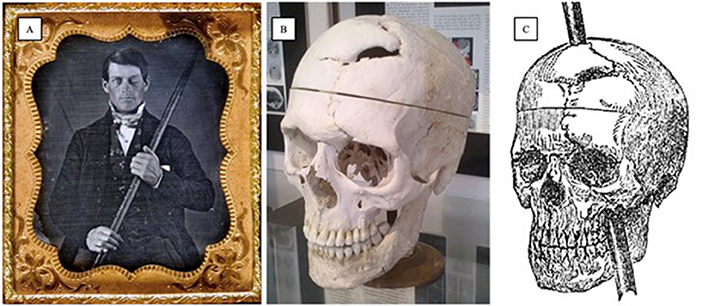
- Figure 1 - (A) A photograph of Phineas Gage holding the tamping rod that shot through his brain.
- [Image credit: Originally from the collection of Jack and Beverly Wilgus, and now in the Warren Anatomical Museum, Harvard Medical School. (https://commons.wikimedia.org/wiki/File:Phineas_Gage_Cased_Daguerreotype_WilgusPhoto2008-12-19_EnhancedRetouched_Color.jpg), Lettering added by R. A. McCurdy, https://creativecommons.org/licenses/by-sa/3.0/legalcode]. (B) Phineas’s skull is currently on display at Harvard University School of Medicine. [Image credit: Van Horn JD, Irimia A, Torgerson CM, Chambers MC, Kikinis R, et al. (https://commons.wikimedia.org/wiki/File:Simulated_Connectivity_Damage_of_Phineas_Gage_SkullDisplayWarren.jpg), https://creativecommons.org/licenses/by/2.5/legalcode]. (C) A drawing showing the rod’s path—entering under the left cheekbone and exiting the top of the skull (Image credit: https://commons.wikimedia.org/wiki/Category:Phineas_Gage).
Phineas was rushed to the hospital and treated by Dr. John Harlow. Despite the terrible injury, Phineas made a remarkable recovery. He could walk, talk, and regained his strength. Yet, Dr. Harlow observed Phineas behaving strangely. Before his accident, Phineas had been kind, hardworking, and organized. After the accident, Phineas was angry, rude, and could not stay organized. He was so different that Dr. Harlow said Phineas Gage was “no longer Gage.” After the injury, Phineas moved around often and worked odd jobs. He died 12 years later, in 1861.
Phineas Gage was the first clear case of changes in personality and thinking skills after frontal lobe injury [1]. The case of Phineas Gage still inspires scientists to learn about the frontal lobe. Scientists study ways to help people recover and live happy lives following frontal lobe damage. Other scientists study how the frontal lobe changes as kids grow up. They study how thinking skills, like staying organized and planning, relate to how kids do in school.
Patients 2 & 3: The Brain and Language (1861–1874)
Is there a place in the brain that controls speech? How would a person communicate if this part of the brain were damaged? Louis Victor Leborgne lost the ability to speak one day. He could only say one word, “tan,” and he would repeat it over and over. Imagine Louis’ frustration! His doctor, Pierre Paul Broca, noticed that, despite Louis’s limited speech, he seemed to understand what others said. He followed simple directions like “close your eyes.” Louis could communicate using gestures and facial expressions. Dr. Broca concluded that Louis was intelligent and could comprehend speech—only his ability to produce speech was affected. After Louis’ death, Dr. Broca studied his brain and found a lesion in the lower left frontal lobe (a different part of the frontal lobe than was damaged in Phineas Gage). Today, this area, which is important for producing speech, is often called Broca’s area (Figure 2) [2].
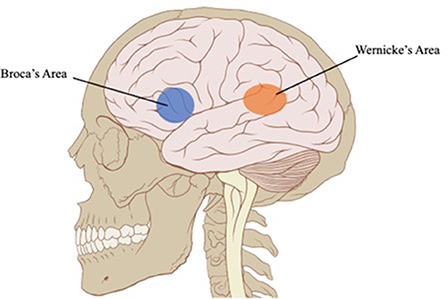
- Figure 2 - Language regions in the brain.
- Broca’s area (blue) is important for producing speech and Wernicke’s area (orange) is important for understanding speech. Both areas are on the left side of the brain (Image credit: Patrick J. Lynch, medical illustrator (https://commons.wikimedia.org/wiki/File:Skull_and_brain_normal_human.svg), “Skull and brain normal human”, Brain region markers by R.A. McCurdy, https://creativecommons.org/licenses/by/2.5/legalcode).
Around the same time, Dr. Carl Wernicke had a patient who became suddenly ill. Susanne Adam could produce speech but could not understand what people said to her—the opposite of Louis. When Susanne spoke, her words sounded made-up. She did not even notice she was making mistakes! Dr. Wernicke discovered that difficulty understanding speech can occur after a lesion in the left temporal lobe. The temporal lobes of the brain are located behind the ears. This area in the left temporal lobe is now called Wernicke’s area (Figure 2) [2]. These early patients taught us that Broca’s area is important for speech production, and Wernicke’s area is important for speech comprehension. Today, we know there are many more areas of the brain that help us talk and communicate—scientists have found a network of brain regions that work together!
Based on their symptoms, Louis and Susanne likely had strokes. Today, healthcare workers called speech-language pathologists help people re-learn to talk after a stroke. Scientists continue to study language by looking at how the brain changes when people recover from strokes. Other scientists study the brains of kids as they learn to talk and read.
Patient 4: The Brain and Memory (1953)
What if you could not make new memories? Is there a difference between old memories and new memories? As a child, Henry Molaison hit his head during a bicycle accident. Shortly after, he started having seizures that made his life hard for many years. When doctors could not stop the seizures with medications, they offered 27-year-old Henry an experimental surgery. Dr. William Beecher Scoville removed the area of Henry’s brain causing the seizures—a part of the temporal lobes that included the right and left hippocampus. He also removed some additional brain tissue around the hippocampus (Figure 3). At first, the surgery seemed successful—Henry’s seizures stopped! However, doctors noticed something unexpected.
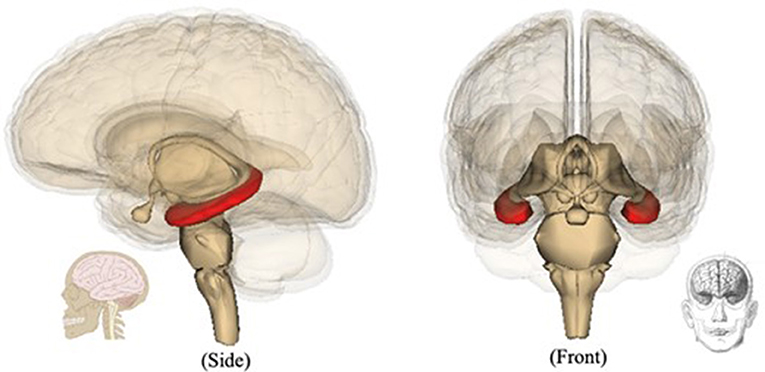
- Figure 3 - Location of the hippocampus (red).
- You have two hippocampi: one on each side of your brain. When the surgeon removed both of Henry’s hippocampi, he was unable to learn new names, faces, facts, and events [Image credit: Images are generated by Life Science Databases (LSDB). (https://commons.wikimedia.org/wiki/File:Hippocampus_image.png), https://creativecommons.org/licenses/by-sa/1.0/legalcode].
Henry seemed confused. He could not tell the doctors what year it was or remember the names of anyone he met after his surgery. He would forget entire conversations almost immediately. Henry seemed unable to make any new memories. The doctors were surprised. They wondered if the hippocampus helped create memories. Dr. Brenda Milner developed many experiments to test Henry’s memory. She discovered Henry could remember things from before his surgery but had trouble learning some types of new information. Scientists call this amnesia, and you can learn more about amnesia in this Frontiers for Young Minds article. Scientists learned a lot from Henry about the hippocampus and memory [3]. Scientists can still study Henry’s brain today. After Henry’s death, a team of scientists froze his brain and cut it into very thin slices. They discovered the exact location of Henry’s brain lesions as well as which areas remained intact [4]. This helped scientists understand some of Henry’s behavioral changes after the surgery and throughout his life.
Scientists continued to study the hippocampus and other brain areas that make memories. They learned how the hippocampus communicates with those brain areas. This knowledge helps today’s researchers study other people with memory disorders. For example, the hippocampus can be damaged in disorders like Alzheimer’s disease and schizophrenia.
Patient 5: The Brain and Fear
What would it be like to live without fear? S.M. (named by her initials to protect her identity) has been called “the woman with no fear.” A rare disorder damaged an area deep inside her brain called the amygdala (Figure 3).
Dr. Ralph Adolphs and his team of scientists conducted an experiment with S.M., exposing her to three frightening experiences and measuring her reactions [5]. First, researchers took S.M. to an exotic pet shop and presented her with snakes and spiders—animals that cause fear in most people. S.M. showed no fear. She let them crawl up and down her arms. She closely examined them and exclaimed how exciting it was. Next, the researchers took S.M. to one of the “most haunted” places in the world: The Waverly Hills Sanatorium, an abandoned hospital. Actors dressed as monsters and hid in dark hallways. S.M. offered to lead the tour group. While other members screamed in terror at the monsters, S.M. smiled, laughed, and even tried talking to them. S.M. said she felt no fear. Instead, she had great fun! In the final experience, S.M. watched movie clips designed to bring out various emotions. Although she smiled and laughed when she saw happy movies, she had no fear response to scary movies.
Based on these experiments, Dr. Adophs’ scientists concluded that the amygdala is important for feeling fear. Scientists today study the role of the amygdala in anxiety disorders and risky behavior. For example, researchers study whether there is a link between the social anxiety observed in some people with autism and differences in their amygdalae.
The Lesion Method Today
The lesion method has improved over time [6]. Single-patient studies like those we have described are great for giving scientists new questions to study, but they cannot answer questions like “is the hippocampus important for memory in most people?” To answer such questions, scientists today study groups of people with similar brain lesions in what are called group lesion studies. These studies can show that lesions to certain parts of the brain are linked to the same behavioral changes for different people. For example, almost all people with damage to the hippocampus have memory difficulties—this is true regardless of age and sex.
The lesion method can be combined with neuroimaging techniques, as you can read about in this Frontiers for Young Minds article. Scientists are learning more about how the parts of the brain work together. For example, there are connections between Broca’s area and Wernicke’s area, and there are also connections between the hippocampus and the amygdala. Combining the lesion method with neuroimaging techniques helps scientists learn how connected parts of the brain work together. This helps scientists understand how brain lesions that damage these connections can change behavior.
The lesion method is still an important tool for studying the brain. A lot of what we know about the brain today started with observations of a single patient. Single patients continue to inspire scientists and teach us about how the brain performs everyday behaviors.
Glossary
Lesion: ↑ An area of the brain that is damaged.
Lesion Method: ↑ A scientific method that studies the relationship between brain and behavior. This method examines changes to behavior following brain damage.
Frontal Lobe: ↑ The part of your brain that sits behind your forehead. It is important for personality and decision-making.
Temporal Lobe: ↑ The part of your brain that sits just behind your ear on both sides of your head. It is important for memory and language.
Hippocampus: ↑ A small part of the brain inside the temporal lobe. It is important for making memories.
Amygdala (uh-MIG-duh-luh): ↑ A small area of the brain in front of the hippocampus. It is important for controlling fear.
Group Lesion Studies: ↑ These scientific studies include many people that all have brain damage (or “lesions”) in the same place of their brains, rather than just one person.
Neuroimaging Techniques: ↑ High-tech methods for scientists to look inside the brain without surgery. Scanners make a computer image of a person’s brain and any lesions in their brain.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Funding was provided by the grant R01 DC017926.
References
[1] ↑ Damasio, H., Grabowski, T., Frank, R., Galaburda, A. M., and Damasio, A. R. 1994. The return of Phineas Gage: clues about the brain from the skull of a famous patient. Science 264:1102–5. doi: 10.1126/science.8178168
[2] ↑ Rutten, G. 2022. “Broca-Wernicke theories: a historical perspective,” in Handbook of Clinical Neurology, Vol. 185, eds A. E. Hillis and J. Fridriksson (Elsevier), p. 25–34. doi: 10.1016/B978-0-12-823384-9.00001-3
[3] ↑ Corkin, S. 2002. What’s new with the amnesic patient H.M.? Nat. Rev. Neurosci. 3:153–60. doi: 10.1038/nrn726
[4] ↑ Annese, J., Schenker-Ahmed, N. M., Bartsch, H., Maechler, P., Sheh, C., Thomas, N., et al. 2014. Postmortem examination of patient HM’s brain based on histological sectioning and digital 3D reconstruction. Nat. Commun. 5:1–9. doi: 10.1038/ncomms4122
[5] ↑ Feinstein, J. S., Adolphs, R., Damasio, A., and Tranel, D. 2011. The human amygdala and the induction and experience of fear. Curr. Biol. 21:34–8. doi: 10.1016/j.cub.2010.11.042
[6] ↑ de Haan, B., and Karnath, H.-O. 2018. A hitchhiker’s guide to lesion-behaviour mapping. Neuropsychologia 115:5–16. doi: 10.1016/j.neuropsychologia.2017.10.021