
Abstract
Multiple sclerosis (MS) is a disease of the brain that renders people unable to do simple day-to-day activities. The cause of MS remains unknown. Doctors hypothesize that there is a “trigger” that makes the immune systems of people with MS overactive, causing injury to their own brains and nerves. Exposure to certain viruses and vitamin deficiencies can increase a person’s likelihood of developing MS. MS causes relatively similar symptoms in children and adults. However, there are specific differences that make the diagnosis, treatment, and outcomes of MS in children unique. Due to these differences, doctors use a special set of criteria (rules) when diagnosing children. There is no cure for MS, but treatments exist to control symptoms and prevent injury to the brain and nerves.
What Parts of the Body Does Multiple Sclerosis Affect?
Multiple sclerosis (MS) affects the brain and spinal cord, which are parts of the nervous system. The nervous system is made up of cells called neurons. Each neuron contains a cell body, dendrites, an axon and a myelin sheath (Figure 1). The cell body acts as the control center for the neuron. The dendrites are extensions that branch out from the cell body to receive signals from the environment or other neurons. Once the dendrites receive a signal, it is sent to the cell body, then, the axon sends the signal to other neurons. The signal travels very slowly through the axon in the absence of a myelin sheath. The myelin sheath is like insulation around a wire—it is a fatty substance that insulates neurons so messages can travel quickly and efficiently between them.
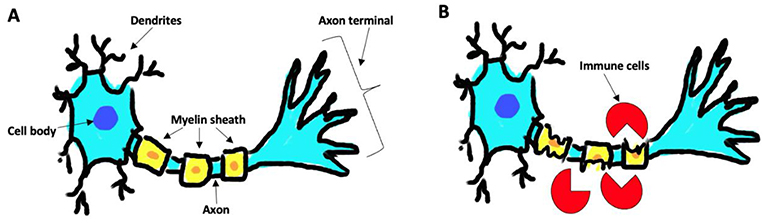
- Figure 1 - (A) A healthy neuron, with an intact myelin sheath, can send signals effectively.
- (B) In MS, immune cells chew up the myelin sheath. Without this insulating substance, signals cannot be sent efficiently from one neuron to another, which results in the various symptoms of the disease.
What Exactly Is MS?
MS is an autoimmune disease. Autoimmune diseases happens when immune cells attack the body by mistake. In MS, immune cells attack the myelin sheath that coats neurons in the brain and spinal cord. Without the myelin sheath, neurons cannot communicate with each other, which makes the body unable to perform important activities. The symptoms of MS depend on which areas of the brain and spinal cord are affected. Symptoms include numbness and weakness in the legs and arms, slurring of words, being off balance, vision issues, and emotional and cognitive changes. Not every person with MS has the same symptoms.
How Is MS in Children Different From Adults?
In the United States alone, nearly one million people are living with MS [1]. MS usually affects people between 20 and 50 years old, but it can impact people younger than 20. If MS is diagnosed in patients who are 18 years old or younger, it is considered pediatric MS.
Before puberty, MS affects boys and girls equally but, after puberty, MS is more prevalent in women (3:1 ratio) [2]. Children are more likely to develop uncommon initial symptoms of MS, which include inflammation of the nerves that control the eye, inflammation of the spinal cord, or acute disseminated encephalomyelitis (ADEM) [2]. ADEM is a disorder that involves swelling of the brain and spinal cord. Some children with ADEM will only have one attack that resolves without happening again. Even if they do not have symptoms again, many children who have ADEM require continued monitoring, to make sure they are not developing MS. In addition to ADEM, kids are more prone to developing tremors and trouble swallowing than are adults with MS, although each patient has unique symptoms.
How do Doctors Diagnose MS in Children?
Doctors diagnose MS in children using the same medical tools that they use with adults. Doctors scan the brain using a technique called magnetic resonance imaging (MRI), and they collect a sample of cerebrospinal fluid (CSF) to analyze it [2]. Even though the tools used to diagnose MS in children and adults are the same, the findings are different.
MS is an immune reaction. When patients receive an MRI scan, they are given a dye that helps the machine create an image. Because areas where immune reactions are happening are active sites of inflammation, they take up the dye quickly, which makes those areas (called lesions) visible on an MRI scan. Children with MS—particularly those less than 12 years old—will present with larger lesions than adults do (Figure 2). The reason for this difference is unknown.
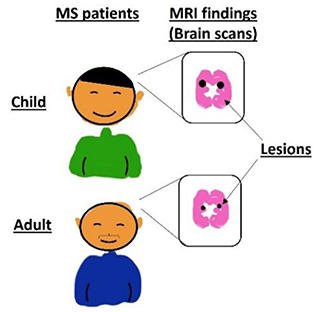
- Figure 2 - MRI scans are used to diagnose MS in both children and adults.
- In children, MS cases often present with larger lesions (black dots) than are seen in adults. The lesions represent areas of inflammation in the brain.
What Causes MS in Children?
We simply do not know yet why children get MS. Risk factors like genetics, exposure to certain viruses, and low vitamin D levels have been linked to a higher likelihood of developing MS as a child. What we do know is that MS is not contagious, so it can not be passed on to other people by contact.
Scientists and doctors believe that genetics play a role in MS. However, no specific genes have been identified as causing MS. Children born to mothers and fathers who have MS have a higher rate of developing the disease, so doctors believe that if a child inherits the correct combination of genes from his or her parents, that child will have a greater likelihood of developing MS [2].
Exposure to the Epstein-Barr virus (EBV) has been reported to increase a child’s chances of developing MS [2]. EBV causes a disease called mononucleosis or, more commonly, “mono.” EBV can trigger the immune system, activating it to cause the symptoms of MS. However, many children who get infected with EBV do not develop MS [2].
Vitamin D deficiency has been shown increase a child’s likelihood of developing MS. Vitamin D is important for keeping the immune system healthy and for brain development [3]. Therefore, it is logical that people who have lower vitamin D levels may be at risk for unhealthy immune responses that could contribute to MS. Because of this finding, physicians have started to prescribe vitamin D supplements to MS patients, to help with symptoms. However, data shows that vitamin D is not always an effective treatment, and the benefits are usually small [3]. In general, most doctors prescribe vitamin D along with other medications, to maximize the chances of controlling symptoms.
How Is MS Treated in Children?
There is currently no cure for MS, but the disease can be treated and managed. There is only one FDA-approved therapy specifically for children with MS, called fingolimod. But MS treatments that are approved for adults are often used for kids [4]. Although many children with MS have low levels of disability, doctors may recommend physical, occupational, or speech therapy to help patients recover [5]. Treatments must be continued over a patient’s entire lifetime, although many therapies significantly decrease the risk of relapses and can help prevent further disability.
To manage flare-ups, children with MS are encouraged to eat a well-balanced diet that includes protein, healthy fats, complex carbohydrates, and lots of greens, to promote their general health. Children are also encouraged to participate in physical activities to increase muscle strength and alleviate symptoms.
Most children with MS who are diagnosed and treated early have minimal symptoms on a day-to-day basis. However, children with MS are more likely than adults to have refractory MS, meaning their MS might not respond to the usual medications. For this reason, children who develop MS need to be cared for by doctors who specialize in this condition. Researchers are currently working on new therapies to reverse the effects of MS.
What Is it Like to Develop MS?
A healthy young woman, a straight-A student and captain of the soccer team, was 16 years old when she developed her first symptoms of MS. Over a few days, she began to notice that her right side felt heavier and heavier, and she began having difficulty moving her legs. These symptoms did not bother her much at first, but 3 days after they started, she fell in her room due to her weakness. Her family took her to her pediatrician who then sent her to the emergency room. There, she met with a neurologist (brain doctor), who performed an MRI of her brain, which showed inflammation. She spent a few days in the hospital taking medicine to help immediately reduce the inflammation. Over the next few weeks, she felt like herself again. She had a long discussion with her neurologist about the treatments she could take to prevent this from happening again. She chose a medicine called natalizumab, which helps block immune cells from moving into the brain. Since starting this medicine, her MRIs have been stable and she has not had any relapses. She graduated from high school last year and is now playing soccer at her university.
Conclusion
Researchers and doctors understand that MS is an autoimmune disease caused by immune cells attacking the myelin sheath of neurons. There are many known risk factors that can trigger MS such as genetics, exposure to the EBV virus and low vitamin-D levels. These are true for MS in both children and adults. However, MS in children presents with larger lesions in the brain and depending on which areas of the brain are affected will determine how severe their symptoms are. Even though MS is a debilitating disease, individuals with MS can still live a meaningful life by managing their disease and flare-ups such as eating a well-balanced diet and getting lots of exercise. Currently, researchers and doctors are working on further understanding the disease as well as developing treatments and possibly a cure in the future.
Additional Resources
https://www.nationalmssociety.org/What-is-MS/Who-Gets-MS/Pediatric-MS
Funding
JR is supported by an MS research grant from the Worcester Foundation for Biomedical Research.
Glossary
Neuron: ↑ Cells that make up the nervous system.
Myelin Sheath: ↑ A fatty substance that wraps around a neuron so messages can travel quickly and efficiently between neurons.
Autoimmune Disease: ↑ A disease where immune cells attack the body by mistake.
Acute Disseminated Encephalomyelitis: ↑ A disorder that involves swelling of the brain and spinal cord.
Magnetic Resonance Imaging (MRI): ↑ An imaging technology that allows doctors to diagnose MS and many other diseases.
Cerebrospinal Fluid (CSF): ↑ Fluid that surrounds the brain and spinal cord.
Refractory MS: ↑ A type of MS where patients do not respond to regularly prescribed MS medications.
Conflict of Interest
JR is an inventor on patent application #62489191, “Diagnosis and Treatment of Vitiligo” which covers targeting IL-15 and Trm for the treatment of vitiligo; and on patent application #15/851,651, “Anti-human CXCR3 antibodies for the Treatment of Vitiligo” which covers targeting CXCR3 for the treatment of vitiligo.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
[1] ↑ Banwell, B., Krupp, L., Kennedy, J., Tellier, R., Tenembaum, S., Ness, J., et al. 2007. Clinical features and viral serologies in children with multiple sclerosis: a multinational observational study. Lancet Neurol. 6:773–81. doi: 10.1016/S1474-4422(07)70196-5
[2] ↑ Ghezzi, A., Baroncini, D., Zaffaroni, M., and Comi, G. 2017. Pediatric versus adult MS: similar or different? Mult Scler. Demyelinating Disord. 2:5. doi: 10.1186/s40893-017-0022-6
[3] ↑ Summerday, N. M., Brown, S. J., Allington, D. R., and Rivey, M. P. 2011. Vitamin D and multiple sclerosis: review of a possible association. J. Pharm. Pract. 25:75–84. doi: 10.1177/0897190011421839
[4] ↑ Chitnis, T., Arnold, D. L., Banwell, B., Brück, W., Ghezzi, A., Giovannoni, G., et al. 2018. Trial of fingolimod versus interferon beta-1a in pediatric multiple sclerosis. N. Engl. J. Med. 379:1017–27. doi: 10.1056/NEJMoa1800149
[5] ↑ Santoro, J. D., Waltz, M., Aaen, G., Belman, A., Benson, L., Gorman, M., et al. 2020. Pediatric multiple sclerosis severity score in a large US cohort. Neurology. 95:e1844–53. doi: 10.1212/WNL.0000000000010414